
Peerless Research·tb-500
TB-500: A Literature Review of the Thymosin Beta-4 Fragment
TB-500 is a synthetic 7-amino-acid fragment of thymosin beta-4. The form sold is not the 43-mer the human trials studied. A cited literature review.
TB-500 has a naming problem that quietly invalidates most of what is said about it. The molecule sold under that name is a seven-amino-acid fragment. The molecule that twenty-five years of human trials actually studied is a protein more than five times its size.
They are not the same compound, and the gap between them is where almost every confident TB-500 claim comes apart. The marketing inherits the parent protein's research record; the vial contains a fragment that has barely been studied on its own.
This review keeps the fragment and the parent in separate columns, maps what the actin biology actually supports, and follows the clinical record where it really leads.
Research content. The article below summarizes published preclinical, in vitro, and clinical research literature on TB-500 (the heptapeptide Ac-LKKTETQ) and its parent protein thymosin beta-4. The compound is sold by Peerless Peptides for laboratory research use only and is not approved by the FDA for human or veterinary administration.
Last reviewed: June 11, 2026 by Peerless Research.
Summary
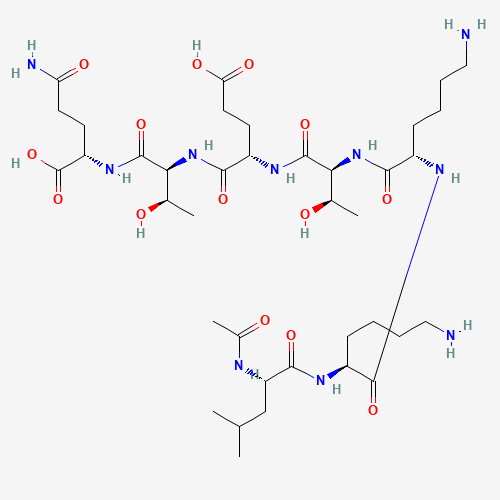
TB-500 is the synthetic acetylated heptapeptide Ac-LKKTETQ, corresponding to residues 17 to 23 of thymosin beta-4, a 43-amino-acid intrinsically disordered protein. The fragment is the form sold for research; the full parent is the form studied in every completed human trial. The parent protein's defining biochemistry, the sequestration of monomeric actin, is well established and partly shared by the fragment. Most of the regenerative claims attached to "TB-500," however, derive from studies of the full protein, and the most prominent of them, cardiac regeneration, has been directly contradicted by independent knockout-mouse work.
The clinical record reinforces the caution. The parent protein has been in human development for about twenty-five years and has missed its pre-specified primary endpoint in each completed Phase 3 trial, after which its developer terminated public reporting. The fragment itself entered its first registered human trial only in 2026. The honest reading is that the actin biochemistry is solid, the human evidence is thin and largely negative, and the form on the market is not the form the evidence describes.
Note: the research described below was conducted in rat and mouse models, in vitro cell systems, and, for the full parent protein only, Phase 1 to 3 clinical trials. Human safety and efficacy of the LKKTETQ fragment specifically have not been established in any peer-reviewed clinical trial. This article is a literature review, not a recommendation of use.
Identity and Chemistry: Two Molecules, One Name
The first discipline TB-500 demands is to separate the fragment from the parent, because commerce and the clinical literature use the same name for two chemically distinct species.
| Commercial "TB-500" | Full thymosin beta-4 | |
|---|---|---|
| Form | Ac-LKKTETQ (7-mer) | 43-amino-acid protein |
| Sequence | Ac-Leu-Lys-Lys-Thr-Glu-Thr-Gln | Ac-SDKPDMAEIEKFDKSKLKKTETQEKNPLPSKETIEQEKQAGES |
| Molecular weight | ~889 Da | ~4,921 Da |
| Formula | C₃₈H₆₈N₁₀O₁₄ | — |
| CAS | 885340-08-9 | 77591-33-4 |
| PubChem CID | 62707662 | 16129704 |
| UniProt | none (synthetic fragment) | P62328 |
The two differ by more than fivefold in mass. The commercial heptapeptide corresponds to residues 17 to 23 of the parent, the conserved actin-binding region plus a terminal glutamine. Full identifiers and per-batch certificates are on the TB-500 product page. Because the heptapeptide contains no aromatic residues, a valid purity reading must be taken by reversed-phase HPLC at 214 to 220 nanometers; a certificate reporting purity at 280 nanometers is measuring the wrong wavelength.
The parent protein was first sequenced from calf thymus by Low and Goldstein in 1981[1]; the same laboratory had sequenced the unrelated immune peptide thymosin alpha-1 four years earlier, a shared name root rather than a shared mechanism. Thymosin beta-4 is intrinsically disordered, holding almost no fixed secondary structure in solution and folding into an extended conformation only when it binds actin. That last point matters for the fragment: a linear seven-residue piece of an already-disordered protein is unlikely to be a structural mimic of the whole, and the literature bears that out unevenly across functions.
Mechanism: One Solid Function, Several Inherited Claims
Thymosin beta-4's defining function is actin sequestration. It is the principal G-actin-sequestering protein in most animal cells, forming a one-to-one complex with monomeric ATP-actin and preventing its polymerization into filaments[2]. Crystallographic and structural work later showed that essentially the entire parent chain wraps the actin monomer, with the LKKTET motif as the central high-affinity contact[3]. The practical consequence is that the LKKTET motif is necessary but not sufficient for full sequestering activity; the flanking residues the fragment lacks contribute to the parent's affinity.
Where the fragment has its own evidence is in angiogenesis-related cell behavior. Philp and colleagues reported that the LKKTET peptide and full thymosin beta-4 showed near-identical activity, at roughly nanomolar concentrations, in endothelial-cell migration and vessel-sprouting assays, and that deleting the motif abolished the effect[4]. This is the single strongest piece of published evidence for the commercial premise that the fragment recapitulates the parent. It is also narrow: it covers in vitro endothelial migration and ex vivo vessel sprouting, not corneal healing, cardiac repair, neuroprotection, or fibrosis.
The parent protein's better-known signaling claims are, on the published record, parent-only. The landmark cardiac paper by Bock-Marquette and colleagues used full-length thymosin beta-4 in a mouse coronary-ligation model and reported activation of integrin-linked kinase and Akt signaling in cardiomyocytes[6]. No published head-to-head shows the heptapeptide reproducing that result.
The same is true for the protein's reported inhibition of NF-κB signaling. The fragment shares the actin contact; it does not automatically inherit the rest.
Preclinical Evidence by System, and Which Molecule Was Used
The thymosin beta-4 literature spans roughly seven tissue systems. Reading it usefully means tracking, in each one, whether the study used the parent protein or the fragment.
Skin. The dermal literature is the only place a direct fragment-versus-parent comparison exists. An early study reported that full thymosin beta-4 was associated with re-epithelialization markers in rodent wounds[14], and a separate paper compared the parent and the LKKTET fragment in diabetic and aged-mouse dermal wounds, the one experiment that puts the heptapeptide directly alongside the protein in an animal model[5]. That single small-animal dermal study is the empirical foundation for the much broader claim that the fragment behaves like the parent everywhere.
Cornea and eye. The most developed clinical application, dry-eye and corneal healing, rests entirely on full-length thymosin beta-4 in its animal and human work[13]. The fragment was not the test article.
Cardiac. This is the system where the strongest claims and the strongest contradictions both live, discussed in the next section.
Central nervous system, tendon, and muscle. The in vivo stroke, brain-injury, and spinal-cord studies used full thymosin beta-4. Tendon and muscle, the systems most heavily invoked in commercial recovery marketing, are the thinnest in the primary literature, and no peer-reviewed rodent tendon study using the isolated LKKTETQ fragment was located in this review.
Fibrosis. The anti-fibrotic story is the cleanest example of why the fragment cannot inherit the parent's reputation. That biology runs through Ac-SDKP, a separate small fragment liberated from the parent's N-terminus, residues 1 to 4. The LKKTETQ heptapeptide, drawn from residues 17 to 23, does not contain that sequence and cannot generate it. Anti-fibrotic claims attached to the commercial fragment are mechanistically misattributed.
A recurring quality caveat applies across systems: group sizes are small, blinding of outcome adjudication is often unstated, and the strongest functional claims rest on single laboratories. The exception is cardiac, where independent groups did engage, and disagreed.
The Cardiac Contradiction
The cardiac claim is the most aggressive in the thymosin beta-4 literature, and the one most directly undermined by independent work.
The optimistic line came from the Smart and Riley group, which reported that the parent protein mobilized epicardial progenitor cells[7] and, in a later paper, that priming with thymosin beta-4 produced new cardiomyocytes from within the injured adult heart[8]. These results drove the molecule's regenerative reputation.
Three independent results pushed back. A lineage-tracing study found that thymosin beta-4 given after myocardial infarction did not reprogram epicardial cells into cardiomyocytes[9]. More fundamentally, two independent knockout-mouse studies showed that animals lacking thymosin beta-4 are born at normal ratios with normal hearts and coronary vessels, which means the protein is dispensable for cardiac development[10][11]. That directly undercuts the claim that it is essential for building the heart's vasculature.
The methodological lesson is specific. Unlike some research peptides, thymosin beta-4 has been studied by many independent groups; the disagreement is not from lack of attention. The groups converge on the actin-sequestration biology and diverge, sharply, on the regenerative reprogramming biology, with the independent knockout data running against the strongest claims.
Clinical Evidence: A Twenty-Five-Year Record of Missed Endpoints
The clinical record is the part of the TB-500 story most often misread as early-stage promise. It is not early-stage. It is a long, mostly negative program, conducted almost entirely with the parent protein.
| Asset (full Tβ4) | Indication | Trial | Primary endpoint |
|---|---|---|---|
| RGN-259 | Dry eye | ARISE-1 (Ph 2/3, n=317) | Missed |
| RGN-259 | Dry eye | ARISE-2 (Ph 3, n=601) | Missed |
| RGN-259 | Dry eye | ARISE-3 (Ph 3, n=700) | Missed (2021) |
| RGN-259 | Neurotrophic keratopathy | SEER-3 (Ph 3, Europe) | Missed |
| RGN-137 | Epidermolysis bullosa | Ph 3 cleared 2017 | No published readout |
| RGN-352 | Acute myocardial infarction | Ph 2 (IV) | FDA clinical hold 2011; never enrolled |
Across roughly twenty-five years and at least three completed Phase 3 trials with disclosed results, the parent protein missed every pre-specified primary endpoint, including the 700-patient ARISE-3. The intravenous cardiac asset never produced human efficacy data, having been placed on clinical hold in 2011 for manufacturing non-compliance. The dermal Phase 3 program was cleared in 2017 and has not reported results since. The developer, RegeneRx, filed to terminate its public-company reporting in August 2023 following the failures.
Earlier Phase 1 work did characterize the parent protein's pharmacokinetics and tolerability in healthy volunteers after intravenous dosing[12], but that was a safety and exposure study, not an efficacy result.
The fragment's own clinical record is shorter still: essentially nonexistent until 2026, when NCT07487363, sponsored by Hudson Biotech, became the first registered human study to use the LKKTETQ heptapeptide by name, in stable cardiovascular disease, with biomarker endpoints. It is recruiting, and no results have been published. The same sponsor is running the first non-originator trial of BPC-157, and the two molecules share the July 2026 advisory-committee docket, but they are mechanistically unrelated, and the published literature contains no controlled study co-administering them. The popular "Wolverine stack" pairing is a podcast-culture artifact, not a research finding.
Research Limitations
Several limitations frame how the TB-500 evidence should be weighted.
The first is the naming gap itself. The fragment sold commercially and the protein studied clinically are different molecules, and the published efficacy record belongs almost entirely to the protein. Any claim that begins "TB-500 was shown to" should be checked against which molecule the cited study actually used.
The second is the inheritance problem. Outside in vitro endothelial migration and one small dermal-wound model, there is no published evidence that the heptapeptide reproduces the parent protein's activity. The corneal, cardiac, neurological, and fibrosis literatures are parent-protein literatures, and the fibrosis biology in particular belongs to a different fragment the heptapeptide cannot generate.
The third is the negative clinical record. The parent protein's twenty-five-year human program missed its primary endpoint in every completed Phase 3 trial. This is not the absence of evidence; it is evidence pointing the other way, at least for the indications tested.
The fourth is an open safety question. Thymosin beta-4 is overexpressed in several metastatic cancers, including melanoma, colon, and breast, and a closely related family member is used as a prostate-cancer metastasis marker. Because cell migration and angiogenesis, the protein's two best-documented activities, are the same processes metastasis exploits, a tumor-interaction question is biologically reasonable. No human trial has been powered to detect a malignancy signal, and the few hundred patients dosed across the parent protein's wound-healing trials would not constitute a meaningful safety study for rare events. Absence of evidence of harm is not evidence of its absence.
None of this makes the molecule inert. The actin-sequestration biochemistry is among the best-characterized in the field, and the fragment genuinely shares the actin-binding motif. The limitations describe how far that established biochemistry can be stretched toward human outcomes, which on the current record is not far.
Regulatory Context
As of June 2026, no TB-500 product is FDA-approved as a drug for any indication. Within the compounding framework, TB-500 was placed on the 503A Category 2 do-not-compound list in September 2023 and removed from it effective April 22, 2026. As with the other peptides in that action, removal is procedural: it does not confer Category 1 status, it is not a finding of safety, and it is not an authorization to compound. The compound remains an unapproved new drug. The distinction between the compounding categories is covered in our 503A vs 503B compounding primer.
The Pharmacy Compounding Advisory Committee reviewed TB-500 on July 23, 2026 under a proposed wound-healing indication, sharing that docket with BPC-157 and other research peptides, and recommended it for the 503A bulks list by a vote of 8 to 6 with one abstention. FDA's own review staff had proposed that it not be added, noting no human studies supporting the nominated indication. A favorable vote on a narrow wound-healing indication does not speak to the musculoskeletal or cardiovascular research interest that draws most attention, and a committee recommendation is not approval. The full outcome is covered in our report on the July 2026 PCAC vote.
In sport, the World Anti-Doping Agency prohibits TB-500 at all times under category S2, with no therapeutic-use exemption available, and anti-doping laboratories have published detection methods for it. The first significant United States enforcement naming TB-500 specifically was a 2023 warning letter to a vendor marketing it as an unapproved drug; unlike BPC-157, TB-500 was not named in the 2020 Tailor Made Compounding plea. The molecule sits in the same regenerative-research cluster as the copper tripeptide reviewed in our GHK-Cu literature review, and the same research-use-only discipline applies to all of them.
References
-
Low TLK, Hu SK, Goldstein AL. Complete amino acid sequence of bovine thymosin β4. Proc Natl Acad Sci USA. 1981;78(2):1162-1166. PMID: 6940133.
-
Safer D, Elzinga M, Nachmias VT. Thymosin β4 and Fx, an actin-sequestering peptide, are indistinguishable. J Biol Chem. 1991;266(7):4029-4032. PMID: 1996337.
-
Irobi E, Aguda AH, Larsson M, et al. Structural basis of actin sequestration by thymosin-β4. EMBO J. 2004;23(18):3599-3608. PMID: 15329672.
-
Philp D, Huff T, Gho YS, Hannappel E, Kleinman HK. The actin binding site on thymosin β4 promotes angiogenesis. FASEB J. 2003;17(14):2103-2105. PMID: 14500546.
-
Philp D, Badamchian M, Scheremeta B, et al. Thymosin β4 and a synthetic peptide containing its actin-binding domain promote dermal wound repair in db/db diabetic mice and in aged mice. Wound Repair Regen. 2003;11(1):19-24. PMID: 12581423.
-
Bock-Marquette I, Saxena A, White MD, DiMaio JM, Srivastava D. Thymosin β4 activates integrin-linked kinase and promotes cardiac cell migration, survival and cardiac repair. Nature. 2004;432(7016):466-472. PMID: 15565145.
-
Smart N, Risebro CA, Melville AAD, et al. Thymosin β4 induces adult epicardial progenitor mobilization and neovascularization. Nature. 2007;445(7124):177-182. PMID: 17495252.
-
Smart N, Bollini S, Dubé KN, et al. De novo cardiomyocytes from within the activated adult heart after injury. Nature. 2011;474(7353):640-644. PMID: 21654746.
-
Zhou B, Honor LB, Ma Q, et al. Thymosin beta 4 treatment after myocardial infarction does not reprogram epicardial cells into cardiomyocytes. J Mol Cell Cardiol. 2012;52(1):43-47. PMID: 21907210.
-
Banerjee I, Zhang J, Moore-Morris T, et al. Cytoskeletal protein thymosin β4 is dispensable for murine cardiac development and function. Circ Res. 2012;110(3):456-464. PMID: 22158707.
-
Rossdeutsch A, Smart N, Dubé KN, Turner M, Riley PR. Essential role for thymosin β4 in regulating vascular smooth muscle cell development and vessel wall stability. Circ Res. 2012;111(4):e89-e102. PMID: 23371905.
-
Ruff D, Crockford D, Girardi G, Zhang Y. A randomized, placebo-controlled, single and multiple dose study of intravenous thymosin β4 in healthy volunteers. Ann N Y Acad Sci. 2010;1194:223-229. PMID: 20536472.
-
Sosne G, Ousler GW. Thymosin β4 ophthalmic solution for dry eye: a randomized, placebo-controlled, Phase II clinical trial. Clin Ophthalmol. 2015;9:877-884. PMID: 25826322.
-
Malinda KM, Sidhu GS, Mani H, et al. Thymosin β4 accelerates wound healing. J Invest Dermatol. 1999;113(3):364-368. PMID: 10469335.
-
NCT07487363, TB-500 (residues 17-23 fragment) for cardiovascular biomarkers in stable atherosclerotic cardiovascular disease (Phase 1/2; sponsor Hudson Biotech; recruiting 2026; estimated n=80). ClinicalTrials.gov.
Not intended to diagnose, treat, cure, mitigate, or prevent any disease. Sold for research, laboratory, or analytical purposes only.
Research Compounds Referenced
The compounds discussed in this article are sold by Peerless Peptides for laboratory research use only. They are not FDA-approved for human or veterinary administration. Per-batch Certificates of Analysis are available.
- TB-500: Synthetic heptapeptide Ac-LKKTETQ, residues 17-23 of thymosin beta-4.PDP entry →
Frequently Asked Questions
- What is TB-500?
- TB-500 is the synthetic acetylated heptapeptide Ac-Leu-Lys-Lys-Thr-Glu-Thr-Gln (Ac-LKKTETQ), corresponding to residues 17 to 23 of the parent protein thymosin beta-4. The seven-amino-acid form is what is sold in research commerce; the full 43-amino-acid parent protein is the form used in published human clinical trials. Confirming the molecular weight on a certificate of analysis (about 889 daltons for the fragment versus about 4,921 for full thymosin beta-4) distinguishes the two. It is sold by Peerless Peptides for laboratory research use only and is not approved by the FDA for human or veterinary use.
- How is TB-500 different from thymosin beta-4?
- They differ by more than fivefold in mass. TB-500 (Ac-LKKTETQ) is a 7-amino-acid synthetic fragment of about 889 daltons; full thymosin beta-4 is a 43-amino-acid intrinsically disordered protein of about 4,921 daltons. The fragment reproduces the actin-binding contact region of the parent but lacks its N-terminal and C-terminal sequences. This distinction is the central one in the TB-500 literature, because the published human clinical trials used full thymosin beta-4, not the fragment.
- Does TB-500 have human clinical trials?
- Essentially none for the fragment itself. Every completed human trial in the thymosin beta-4 record used the full 43-mer parent protein, and that program missed its pre-specified primary endpoint in each of its completed Phase 3 trials over roughly 25 years. As of mid-2026, NCT07487363 (Hudson Biotech) is the first registered human study using the LKKTETQ 7-mer by name, and it is recruiting; no results have been published.
- Is TB-500 FDA approved?
- No. TB-500 is sold strictly for laboratory research use only and has not been evaluated by the FDA for any human or veterinary indication. It was removed from the FDA 503A Category 2 do-not-compound list effective April 22, 2026, but removal does not confer Category 1 status or compoundability. The Pharmacy Compounding Advisory Committee reviewed TB-500 on July 23, 2026 on a proposed wound-healing indication and recommended it for the 503A bulks list, 8 to 6 with one abstention, against FDA staff's written position. A Committee recommendation is advisory and does not authorize compounding; rulemaking would still be required. The World Anti-Doping Agency prohibits it at all times under category S2.
- What does the research on TB-500 show?
- The actin-sequestration biochemistry of the parent protein is well established, and the fragment shares the actin-binding contact region. Beyond that, most reported activity (cardiac, corneal, neurological, fibrosis) comes from studies of the full parent protein, and several of the strongest regenerative claims, particularly in the heart, have been directly contradicted by independent knockout-mouse studies. The published human efficacy record for the parent protein is a series of failed Phase 3 trials; the fragment has no published efficacy record at all.